
Remdesivir in Adults With Severe COVID-19: A Randomised, Double-Blind, Placebo-Controlled, Multicentre Trial
Lancet 2020; 395(10236):1569-1578
Epub April 29, 2020
Yeming Wang, Dingyu Zhang, Guanhua Du, Ronghui Du, Jianping Zhao, Yang Jin, Shouzhi Fu, Ling Gao, Zhenshun Cheng, Qiaofa Lu, Yi Hu, Guangwei Luo, Ke Wang, Yang Lu, Huadong Li, Shuzhen Wang, Shunan Ruan, Chengqing Yang, Chunlin Mei, Yi Wang, Dan Ding, Feng Wu, Xin Tang, Xianzhi Ye, Yingchun Ye, Bing Liu, Jie Yang, Wen Yin, Aili Wang, Guohui Fan, Fei Zhou, Zhibo Liu, Xiaoying Gu, Jiuyang Xu, Lianhan Shang, Yi Zhang, Lianjun Cao, Tingting Guo, Yan Wan, Hong Qin, Yushen Jiang, Thomas Jaki, Frederick G Hayden, Peter W Horby, Bin Cao, Chen Wang
PMID: 32423584
DOI: 10.1016/S0140-6736(20)31022-9
ClinicalTrials.gov: NCT04257656
Introduction
On the 31st of December, 2019, Wuhan Municipal Health Commission reported cases of atypical pneumonia linked to a new coronavirus. The disease was later named COVID-19 and the coronavirus SARS-CoV-2. As of now (May 22, 2020), the virus has spread to more than 200 countries infecting more than 5,260,000 people. As a result, this has prompted a race to find effective treatment in order to reduce mortality and ease economic burden on the countries grappling with the new nemesis. Various treatment options have already been tested in clinical trials, with many still ongoing. One of the candidates is remdesivir, an antiviral originally developed to treat hepatitis C and tested against Ebola. A Trial of Remdesivir in Adults With Severe COVID-19 (NCT04257656) is the first published, randomised, placebo-controlled trial of remdesivir in patients with COVID-19.
SARS-CoV-2
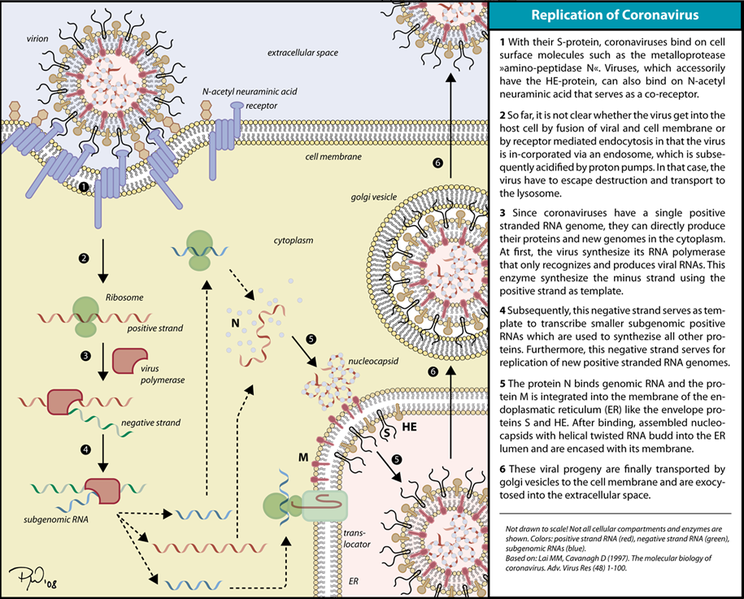
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a betacoronavirus closely related to SARS-CoV (more so than MERS-CoV). As all coronaviruses, it is an enveloped positive-stranded RNA virus. Its replication cycle is shown in the graphics below. Main point is that the virus uses RNA-dependent RNA polymerase to replicate and this is the mechanism of action of remdesivir.
What is remdesivir
Remdesivir is a pro-drug of a ribonucleotide analog with broad spectrum antiviral activity in vitro against filoviruses, pneumoviruses, paramyxoviruses and coronaviruses. After conversion into active metabolite, remdesivir works as a ribonucleotide analog. It interferes with the action of viral RNA polymerase and decreases production of viral RNA via irreversible termination of replicating RNA chain. Known side effects include increase in ALT and AST and nonspecific infusion related reactions like hypotension, nausea and vomiting and sweating.
As mentioned, remdesivir has been proven to have effect in in vitro models against multiple viruses. In vivo activity has been demonstrated in animal models with SARS-CoV and MERS-CoV and now there are emerging trials of its use in animal models and humans with SARS-CoV-2 and COVID-19.
Methods
Study design
This was a randomised, double-blind, placebo-controlled, prospective, multicentre trial conducted at 10 hospitals in Hubei, China, which is definitely the appropriate type of trial. Eligible patients were assigned in a 2:1 ratio and the randomisation was stratified according to respiratory support.
Did the trial address a clearly focused issue?
Yes. Purpose of the study was to evaluate efficacy and safety of remdesivir in hospitalised patients with COVID-19 by observing time to clinical improvement on a six-point ordinal scale.
Was the assignment of patients randomised?
Yes in 2:1 ratio.
Were patients, health workers and study personnel ‘blind’ to treatment?
Yes.
Inclusion criteria
- Men and non-pregnant women aged 18 and above
- SARS-CoV-2 RNA detected on RT-PCR
- Lung involvement on chest imaging
- SpO2 of ≤94% on room air or Pa02/Fi02 ratio <300mgHg
- Onset of symptoms in the previous 12 days
Exclusion criteria
- Severe liver disease
- Pregnancy or breastfeeding
- Renal impairment (eGFR ≤30 mL/min) or dialysis
Procedures
Patients in the treatment group received 200 mg of intravenous remdesivir on day 1, followed by 100mg once daily for up to 10 days, whereas patients in the control group received the same volume of placebo infusions. They were assessed every day using cards with a six-category ordinal scale:
- discharge;
- hospital admission, not requiring oxygen support;
- hospital admission, requiring oxygen support;
- hospital admission, requiring high-flow nasal cannula or non-invasive mechanical ventilation;
- hospital admission, requiring invasive mechanical ventilation or extracorporeal membrane oxygenation;
- death.
Follow-up
Follow up period was 28 days, or until death or discharge, whichever came first.
Were all of the patients who entered the trial properly accounted for at its conclusion?
No. Patients who didn’t clinically improve within 28 days or died were considered as right censored on day 28.
Endpoints
The primary endpoint was defined as time to clinical improvement specified as the improvement by two categories on the six-category ordinal scale, or the patient was discharged alive.
The secondary endpoints were:
- all-cause mortality;
- percentage of patients in each of the categories at day 7,14, and 28;
- incidence of invasive mechanical ventilation;
- duration of oxygen therapy;
- duration of hospital admission;
- and proportion of patients with nosocomial infection.
Were the groups similar at the start of the treatment?
The 2 groups were relatively similar given that only 233 patients were assigned in the trial. However, the prevalence of cardiovascular comorbidities (hypertension, coronary artery disease, diabetes) was higher in the remdesivir group.
Aside from the experimental intervention, were the groups treated equally?
The percentage of patients receiving injections of interferon alpha-2b was higher in the placebo group (38% compared to 29%), but apart from that, yes.
Results
There was no statistically significant difference between the two groups either in terms of primary or in terms of secondary endpoints; all elements’ confidential intervals included either 1 or 0. Time to clinical improvement in the remdesivir group was 21.0 days vs 23.0 days in the placebo group, HR 1.23 [95% CI 0.87-1.75]. 28-day mortality and other secondary endpoints were statistically insignificant as well. However, authors tended to mention that some numerical variances existed between the groups.
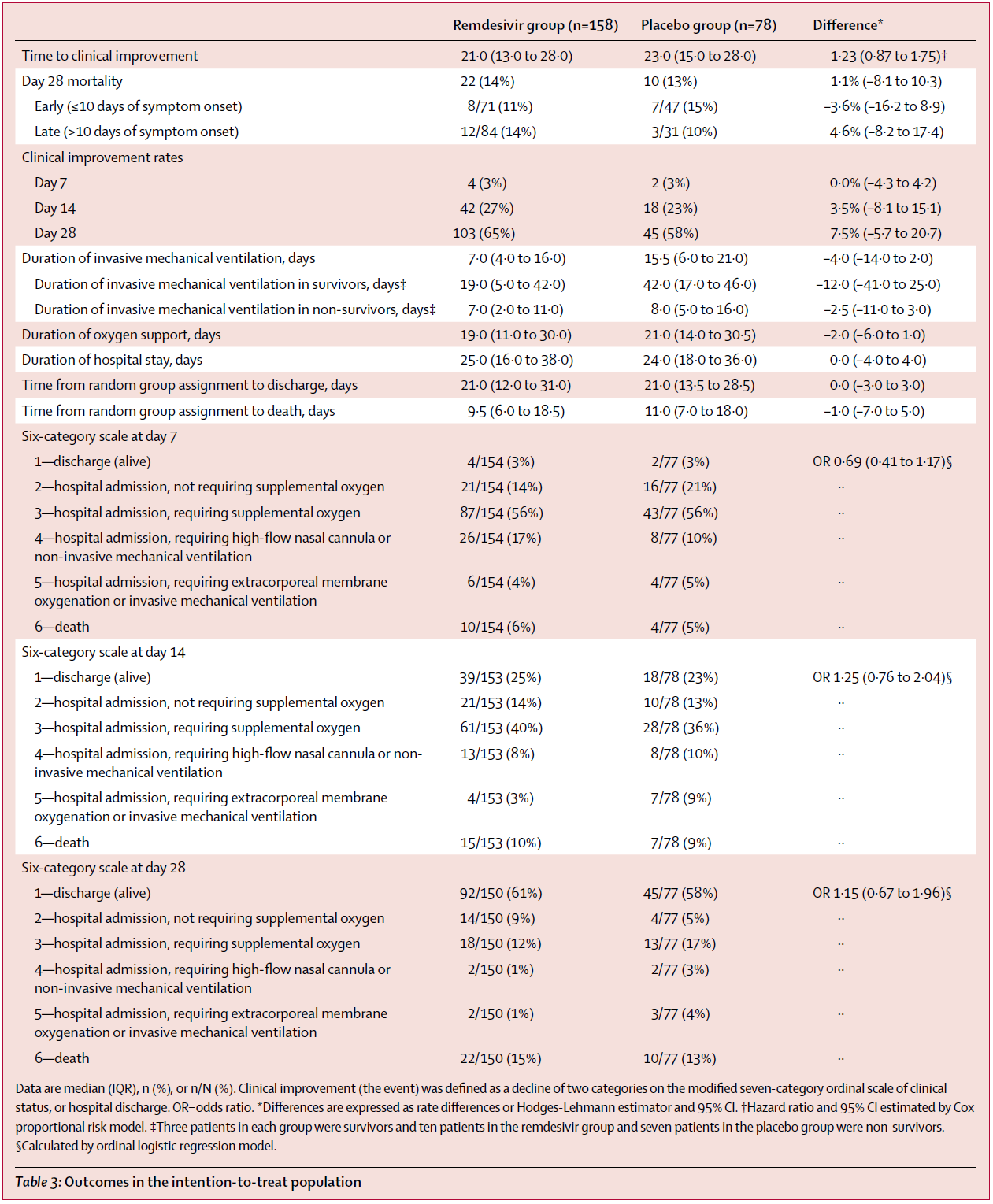
I think it’s important to highlight that the trial was stopped early due to lockdown restrictions which led to lower incidence and insufficient enrollment. It was estimated that 325 patients were needed to have enough statistical power while only 233 were involved. Nonetheless, this doesn’t change anything on the conclusion that, in this study, remdesivir was not superior to placebo when treating patients with severe COVID-19.
How large was the treatment effect?
There was no statistically significant effect.
How precise was the estimate of the treatment effect?
Study was underpowered due to insufficient enrollment.
Discussion
This is the first published randomised placebo-controlled study of remdesivir in patients with severe COVID-19 (i.e. requiring oxygen and hospitalisation) and it comes soon after a controversial compassionate use of remdesivir. It was well designed, randomised and stratified. However, it still has not proved any significant benefit of remdesivir (on limitations see below).
In the compassionate use published in NEJM total of 53 patients were given remdesivir with no control group to compare. In 68% (n=36) of patients clinical improvement was observed and 13% (7 patients) died. Patient population was more ill as 64% patients (n=34) was on invasive ventilation at baseline. No conclusions can be drawn from this study due to multiple reasons but mainly due to no control group.
In contrast, Adaptive COVID-19 Treatment Trial (ACTT) sponsored by NIAID has shown more promise with their preliminary data. This randomised, double-blined, placebo-controlled trial with 1063 patients is running from February 21. Data were preliminary analysed on April 27 showing promising results. Patients who received remdesivir had a statistically significant 31% faster time to recovery than those on placebo (p<0.001). with a median of 11 days compared to 15 days, respectively. Although there is numerically lower mortality in the remdesivir group, statistical significance has not been proven (p=0.059).
Benefit of remdesivir might not be in lowering mortality or viral load but in faster time to recovery and shorter hospital stay. This resembles oseltamivir in treatment of influenza.
Limitation of the study by Wang, et al., same as in the compassionate use, is use of the remdesivir relatively late in the disease course. Here, the earliest use of remdesivir from symptom onset was 9 days with a median of 11 days. It is around this time when complications like sepsis and ARDS develop and patients are transferred to ICU for ventilation, as shown in this study by Zhou et al. It is possible that by this time inflammation and organ damage might be so extensive that reducing viral load with remdesivir might not translate into favourable clinical outcomes. In animal models it is early (within 24 hours of virus infection) use of remdesivir that has reduced viral load (see comparison with animal studies by PulmCrit). There is a possibility that earlier use of remdesivir might have more impact on clinical severity or course of the disease. Obviously, this needs to be investigated further.
On May 12 National Institutes of Health in the United States updated their guidelines on treatment of COVID-19 and now recommend use of “remdesivir for the treatment of COVID-19 in hospitalised patients with severe disease, defined as SpO2 ≤94% on ambient air (at sea level), requiring supplemental oxygen, mechanical ventilation, or extracorporeal membrane oxygenation”. In mild and moderate COVID-19 use of remdesivir is not recommended.
Can the results be applied to the local population, or in your context?
No. It has been revealed in the literature that some racial, socioeconomic and other factors might play a role in the prognosis. This study was conducted in a specific area of China on a relatively small group of patients while socioeconomic and racial characteristics haven’t even been disclosed. Given the abundance of patients worldwide and the severity of the pandemic, it shouldn’t be difficult to conduct a multi-national study.
Were all clinically important outcomes considered?
Time to improvement and level of support, mortality, and length of hospital stay have been considered. Longer follow-up period will be needed to consider clinical outcomes in convalescence period.
Are the benefits worth the harms and costs?
Remdesivir appears to have not so severe side effects and can be considered safe. However, it remains for the most part an experimental drug and its cost is not yet established. Benefits have not yet been well demonstrated, although preliminary data from ACTT look promising.
Many more RCTs of therapeutics for COVID-19 are currently being conducted and will soon be published. One of them is lopinavir/ritonavir and you can expect its critical appraisal soon.
Author and attribution
Tomáš Babišík is Junior Clinical Fellow at St Helens and Knowsley Teaching Hospitals NHS Trust. No conflicts of interest have been disclosed.
Timotej Vataha is a trainee physician in the Internal Medicine Training programme in the UK. No conflicts of interest have been disclosed.
Questions from RCT checklist by Critical Appraisal Skills Programme have been used under non-commercial CC 3.0 license.
References
“Coronavirus Update (Live): 5,265,602 Cases and 337,983 Deaths from COVID-19 Virus Pandemic – Worldometer”. (n.d.). , available at: https://www.worldometers.info/coronavirus/ (accessed 22 May 2020).
Grein, J., Ohmagari, N., Shin, D., Diaz, G., Asperges, E., Castagna, A., Feldt, T., et al. (2020), “Compassionate Use of Remdesivir for Patients with Severe Covid-19”, New England Journal of Medicine, Vol. 0 No. 0, p. null.
“NIH Clinical Trial Shows Remdesivir Accelerates Recovery from Advanced COVID-19 | NIH: National Institute of Allergy and Infectious Diseases”. (n.d.). , available at: http://www.niaid.nih.gov/news-events/nih-clinical-trial-shows-remdesivir-accelerates-recovery-advanced-covid-19 (accessed 22 May 2020).
Pulmonary, S.M.F. is the creator of P. org H. is an associate professor of and Vermont, C.C.M. at the U. of. (2020), “PulmCrit – Eleven reasons the NEJM paper on remdesivir reveals nothing”, EMCrit Project, 11 April, available at: https://emcrit.org/pulmcrit/pulmcrit-eleven-reasons-the-nejm-paper-on-remdesivir-reveals-nothing/ (accessed 22 May 2020).
“Remdesivir (United States: Investigational agent; refer to Prescribing and Access Restrictions): Drug information – UpToDate”. (n.d.). , available at: https://www.uptodate.com/contents/remdesivir-united-states-investigational-agent-refer-to-prescribing-and-access-restrictions-drug-information?topicRef=127429 (accessed 22 May 2020).
Wang, M., Cao, R., Zhang, L., Yang, X., Liu, J., Xu, M., Shi, Z., et al. (2020), “Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro”, Cell Research, Vol. 30 No. 3, pp. 269–271.
Wang, Y., Zhang, D., Du, G., Du, R., Zhao, J., Jin, Y., Fu, S., et al. (2020), “Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebo-controlled, multicentre trial”, The Lancet, Vol. 395 No. 10236, pp. 1569–1578.
“WHO Timeline – COVID-19”. (n.d.). , available at: https://www.who.int/news-room/detail/27-04-2020-who-timeline—covid-19 (accessed 22 May 2020).
Wikipedia. (2020), “Remdesivir”, 21 May, available at: https://en.wikipedia.org/w/index.php?title=Remdesivir&oldid=957943219 (accessed 22 May 2020).

