A Comparison of Two LDL Cholesterol Targets after Ischemic Stroke
N Engl J Med 2020; 382:9-19
January 2, 2020
Amarenco P, Kim JS, Labreuche J, Charles H, Abtan J, Béjot Y, Cabrejo L, Cha JK, Ducrocq G, Giroud M, Guidoux C, Hobeanu C, Kim YJ, Lapergue B, Lavallée PC, Lee BC, Lee KB, Leys D, Mahagne MH, Meseguer E, Nighoghossian N, Pico F, Samson Y, Sibon I, Steg PG, Sung SM, Touboul PJ, Touzé E, Varenne O, Vicaut É, Yelles N, Bruckert E; Treat Stroke to Target Investigators.
PMID: 31738483
DOI: 10.1056/NEJMoa1910355
ClinicalTrials.gov: NCT01252875
Due to SARS-CoV-2 pandemic we have suspended Twitter session for this topic until further notice to bring you more COVID-19 related information.
Background
Although lipid-lowering therapy is recommended after transient ischaemic attack (TIA) or ischaemic stroke of atherosclerotic origin, low-density lipoprotein (LDL) cholesterol target levels have not been well studied, whereas recommendations of proportional reductions are more common. Therefore, this article studied risks of cardiovascular events in two LDL target groups following the above-mentioned afflictions.
What do NICE guidelines say?
Unless contraindicated, treatment with a high intensity statin (such as atorvastatin 20-80mg daily) will be offered at diagnosis of ischaemic stroke or TIA by secondary care. The aim of statin therapy is to reduce non-HDL cholesterol by more than 40%.
If the reduction is not achieved within 3 months, consider adherence, diet, lifestyle, and increasing dose (if appropriate).
Fibrates, bile acid sequestrants, nicotinic acid and omega-3 fatty acid compounds should not be prescribed to people with ischaemic stroke or TIA for secondary vascular prevention. Ezetimibe should only be used in patients who also have familial hypercholesterolemia.
Methods
Study design & Funding
This was a randomised, prospective, parallel-group, event-driven trial conducted at 61 sites in France and 16 sites in South Korea.
The prime funds came from French Ministry of Health and SOS-Attaque Cerebrale Association. However, grants from Pfizer, AstraZeneca and Marck were unrestricted.
Eligibility
Patients with ischaemic stroke in the last 3 months, whose deficit was stable and their modified Rankin score was between 0 to 3 indicating they either had no deficit at all (score 0), no disability (score 1), or needed assistance with daily activities (score 2 and 3). Those with score 4 or 5 indicating being dependent or bedridden were excluded. An ischemic stroke was defined as symptoms with a documented ischemic lesion on computed tomography (CT) or magnetic resonance imaging (MRI) in the cerebral regions corresponding to the symptoms, even if the symptoms were transient. Patients with TIA in the last 15 days were also eligible, with TIA defined as a motor deficit in at least one arm or leg or a slurred speech lasting more than 10 minutes.
The cut-off age was 18 (18 and older could have been enrolled) in France and 20 in South Korea.
As recommended by AHA-ASA guidelines, all patients were screened with a use of non-invasive imaging of cervical vessels as a part of routine evaluation. Other types of imaging were also used in order to identify signs of atherosclerosis. Choice of imaging was not randomized. All eligible patients had atherosclerotic disease that included stenosis of an extracranial or intracranial cerebral artery, ipsilateral or contralateral to the region of imputed brain ischemia; atherosclerotic plaques of the aortic arch measuring at least 4 mm in thickness; or a known history of coronary artery disease.
- Ischaemic stroke in previous 3 months with stable deficit and modified Rankin score of 0 to 3 or TIA in previous 15 days
- Age of 18 or above in France, 20 or above in South Korea
- Atherosclerotic disease demonstrated on non-invasive imaging of a non-randomized choice
Were all eligible patients offered to be a part of the trail?
Not clear.
This is not clear whether the patients having come to the study sites were all considered to be eligible at first until having been ruled out. However, what’s mentioned is that 13 did not sign a consent form and were, therefore, excluded.
Did the study address a clearly focused issue?
Yes.
Total of 2860 patients were enrolled prospectively and followed up for a median of 3.5 years with 1430 patients in each group. The mean achieved LDL cholesterol level was 65 mg per decilitre (1.7 mmol per litre) in the lower-target group and 96 mg per decilitre (2.5 mmol per litre) in the higher-target group. Primary end-points were clearly defined and results were evaluated by a central adjudication committee.
Was the assignment of patients to treatments randomised?
Yes. The eligible patients were randomly assigned in a 1:1 ratio.
Were patients, health workers and study personnel ‘blind’ to treatment?
No.
Although adjudicators were unaware of LDL cholesterol targets and levels, the investigators and the technical and clinical research assistants were aware of the assigned targets. This might have caused that the percentage of time patients spent in the assigned therapeutic range of LDL cholesterol was 52.8% in the lower-target group (53.4% among the French patients and 50.8% among the Korean patients) and 32.2% in the higher-target group (33.1% and 29.1%, respectively, for each country). Bias?
Were the groups similar at the start of the trail?
Yes.
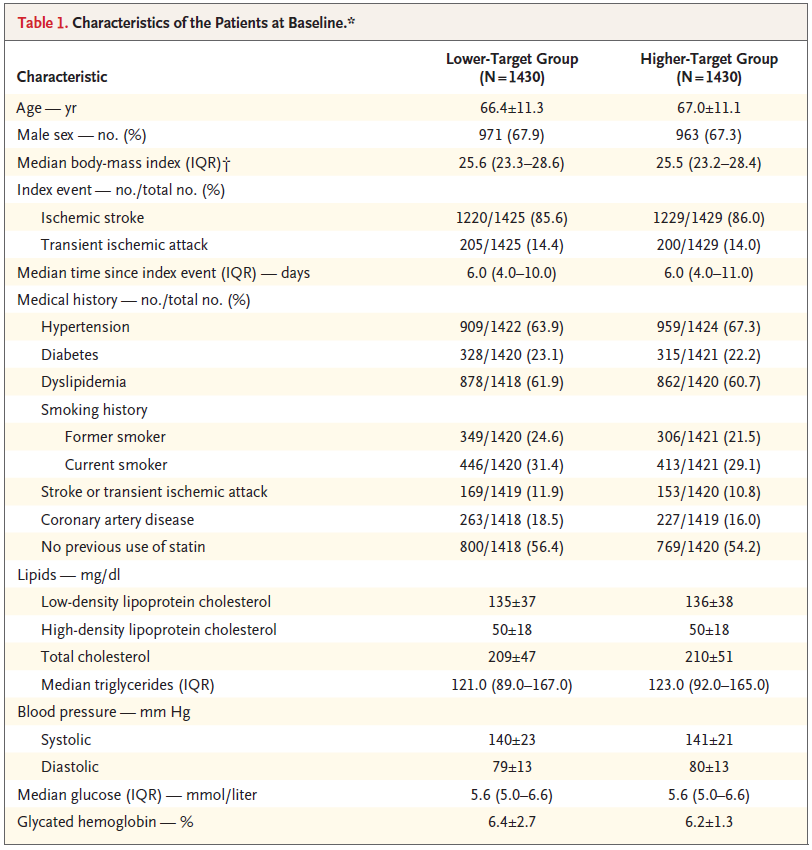
As it can be seen, both groups are very similar in all the elements mentioned in the table above.
Were the groups treated equally aside from the intervention?
Yes.
Levels of triglycerides, HDL cholesterol, blood pressure in the sitting position, fasting glucose and glycated haemoglobin were monitored and recommendations regarding their management were given. Additionally, smoking cessation was encouraged.
Were all the patients who entered the trial properly accounted for at its conclusion?
Yes.
Was the follow up long enough?
No.
It was estimated that enrollment of 3876 patients would result in 385 primary end-point events, with a power of 80% to detect a 25% lower relative risk in the lower-target group. The trial was prematurely stopped due to lack of funding with 2870 patients (which are all the patients entering the trial) and 277 primary end-point events.
Results
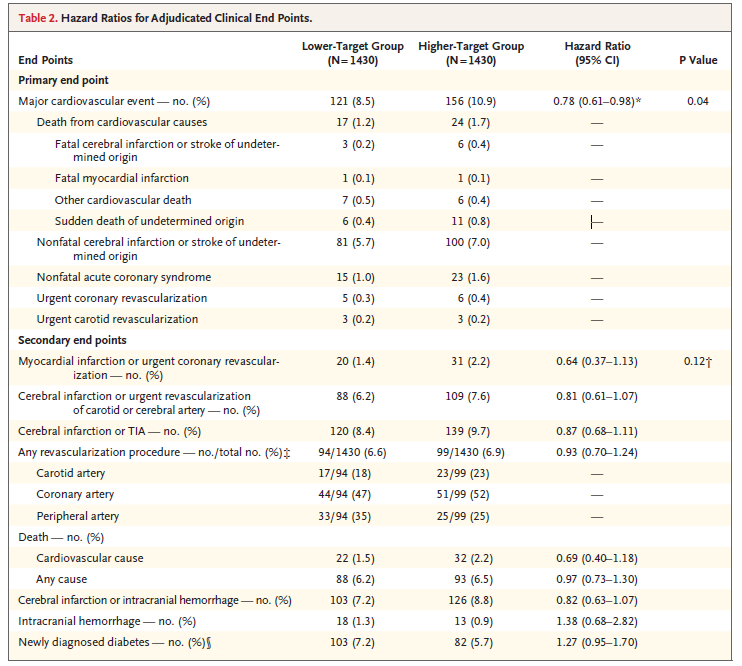
The end points are divided to the primary and secondary endpoints.
The primary end point is defined as a ‘major cardiovascular event’ comprising:
- death from cardiovascular causes
- nonfatal cerebral infarction or stroke of undetermined origin
- nonfatal acute coronary syndrome
- urgent coronary or carotid revascularization
The secondary end points comprise:
- myocardial infarction
- cerebral infarction, TIA, intracranial haemorrhage
- any revascularization (carotid, coronary, or peripheral artery)
- newly diagnosed diabetes
- death from any cause
The occurrence of the elements included in the major cardiovascular events group showed a statistically significant reduction in the lower target group. However, the hazard ratios for all secondary end-point events were generally in the same direction as the hazard ratio for the primary end point, but the confidence intervals all included 1.00, including those for stroke and TIA, making it statistically insignificant.
Are the results similar to other available evidence? Yes.
As mentioned in the article:
“A subsequent analysis of the data from SPARCL trial showed that patients who reached a level of LDL cholesterol of less than 70 mg per deciliter (1.8 mmol per liter) had a 28% lower relative risk of stroke than those who reached a level of 100 mg per deciliter (2.6 mmol per liter).”
P. Amarenco et al. (2020)
“A meta-regression analysis, including results from the SPARCL trial, showed that the risk of stroke was 20% lower for every reduction of 39 mg per deciliter (1.0 mmol per liter) in the LDL cholesterol level, without any threshold effect.”
P. Amarenco et al. (2020)
Discussion
The group of patients was fairly numerous and the study design with data gathering and processing appropriate which gives this article high credibility. However, the fact it was prematurely terminated might have added to the weaknesses of the results, with no secondary end point being statistically significant. Moreover, the choice of the elements included in the primary end points has not been explained and might seem tailored. Additionally, the results cannot be applied to the whole population due to the eligibility criteria – the patients with severe neurological deficit were excluded and in order to achieve the lower target-group cholesterol level, around a third of the patients were commenced on ezetimibe which, in the UK, is reserved for the patients with familial hypercholesterolemia. In addition, cost-effectiveness of this intervention hasn’t been assessed in this study.
To conclude, I don’t think that this study has the strength to change guidelines due to the facts mentioned above.
Further notes
No information regarding compliance with the 6-monthly visits was provided.
Median follow-up was 2.0 years in South Korea and 5.3 years in France, which probably makes the results not applicable for the South Korean population.
Intracranial bleeding was noted as an adverse effect. There was a numerically higher number in the lower target group, however, not statistically significant and information regarding the use of warfarin or DOACs in both groups is not available. Nonetheless, this was also noted in previous studies, therefore, my opinion is that appointing of a safety monitoring committee might be appropriate.
Are there any similar studies being conducted at the moment?The Effect of InTensive Statin in Ischemic Stroke With inTracranial Atherosclerotic Plaques (INSIST-HRMR), Hui-Sheng Chen, General Hospital of Shenyang Military Region, estimated completion: Nov, 2021
Study on Rosuvastatin+Ezetimibe and Rosuvastatin for LDL-C Goal in Patients With Recent Ischemic Stroke, multiple sites in South Korea, estimated completion: Nov, 2020
Author and attribution
Tomáš Babišík is Junior Clinical Fellow at St Helens and Knowsley Teaching Hospitals NHS Trust. No conflicts of interest have been disclosed.
Questions from RCT checklist by Critical Appraisal Skills Programme have been used under non-commercial CC 3.0 license.
References
Critical Appraisal Skills Programme (2018). CASP Checklist. [online] Available at: https://casp-uk.net/wp-content/uploads/2018/03/CASP-Randomised-Controlled-Trial-Checklist-2018_fillable_form.pdf?fbclid=IwAR1qx2uRJjyy1BwOnP1zK13q3cVIAiA4E-YrnwfOAkuWWo9psJqjDpFNHWU. Accessed: January, 2020.
Nice.org.uk. (2019). Stroke and TIA | Guidance | NICE. [online] Available at: https://cks.nice.org.uk/stroke-and-tia#!management Accessed: January. 2020.
P. Amarenco et al. (2020). A Comparison of Two LDL Cholesterol Targets after Ischemic Stroke. Available at: https://www.nejm.org/doi/full/10.1056/NEJMoa1910355 Accessed: January. 2020.

